
It's that time of the year - you have completed your residency interviews, celebrated the completion of a major milestone that you have no intentions of revisiting and now are gearing up to create the ultimate Rank Order List (ROL) that will determine where you spend the next 3-5 years of your professional career in graduate medical education.
So why is it so difficult? Why does it sound so complicated? Why do medical graduates get anxiety attacks just by thinking abou the ROL? Why do medical graduates dread creaing the ROL, knowing fully well that it's important to think through all the options?
Let's understand why this is. Just try shopping on Amazon for 'android phone' and you get millions of options. And what is the most common response then? You close the website hoping to revisit it in the future. How do you then narrow down to choosing that one phone? This is called 'analysis paralysis'.
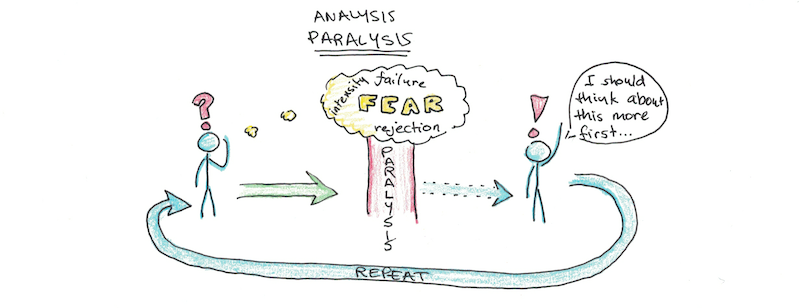
You see, it's because there are so very many possibilities, no one has a way to know what is the right ROL that is perfect for YOU. The stress of missing out on the right one is just too much for some to bear. Remember iPhones? Apple has kept it product line to 2-3 models and is much simpler to choose from and buy.
Still don't believe me? Let's look at an example.
Let's assume there are 3 internal medicine programs that you interviewed at and are trying to rank:
Emory University, Atlanta GA
University of Connecticut, Hartford CT
William Beaumont Hospital, Royal Oak MI
Now before we proceed to rank these programs, let me tell you that what I am going to discuss next are purely my opinions and are in no way trying to tell you which program is better or worse and that you need to use your sound judgment and research when creating your ROL.
Now if you have 3 programs, mathematically there are 6 possible ROL's. Which applicant opts for which ROL depends entirely on 'What's important for him/her'.

For an applicant, if the allure of fellowship opportunities or name/Prestige of the hospital is important [ie the name of the hospital should contain "University"], then that applicant is likely to rank Emory University as 1st, University of Connecticut the 2nd and William Beaumont Hospital as 3rd.
If the applicant is an international medical graduate seeking an H1 B visa, think that applicants rank order list is likely to be Emory 1st, Beaumont 2nd and University of Connecticut 3rd.
If the applicant likes variety and exposure to different hospitals with different healthcare systems and EMR and patient population then that applicants rank order list is likely to be UConn first, Emory second and Beaumont third.
If the applicant has family in the Northeast or lumps no then that applicant would prefer programs in northern part of US and the rank order list would then be likely UConn first, Beaumont second and Emory third [no snow in Atlanta].
If the applicant prefers small class size and collegial LAT from interactions between the residents and attendings and does not want to be in a big city with high cost of living or deal with traffic then that applicants rank order list is likely to be Beaumont first, UConn second and Emory third.
Lastly if the applicant is a cardiology freak and wants to work in the best interventional cardiology centers with liters and cardiology and has an eye for participating in ground breaking cardiology research trials, and that applicants rank order list is likely to be Beaumont first, Emory second and UConn third.
So the bottom line of this exercise is that a ROL is very personal and no one but YOU alone can create and justify your very own ROL. - Dr Ed.
What are the criteria or tools that can help me rank the programs? I will be discussing this in my next post. Subscribe to this blog at www.ed4medus.com to stay updated on latest information and posts by me. Also, check out my Facebook group Facebook.com/groups/Ed4medUS/to interact with other applicants like you, post questions, obtain answers and share your knowledge wealth.
Photo credits:
https://cdn.clipart.email/742ac8277920579388c0a3aeb6807dd0_pulling-hair-out-cartoon-group-16-_1280-720.jpeg
https://www.scotthyoung.com/blog/wp-content/uploads/2019/01/paralysis-001.png
https://encrypted-tbn0.gstatic.com/images?q=tbn:ANd9GcRy13DlFh5EdaB3KxfEo_BKJG0tEn7PxCdCduJaHSm5ZDHUOM1p&s


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}